Intranasal
IN fentanyl
2 mcg/kg
Max 100 mcg
Northwell Health
Emergency Medicine
XR recognition, classification, and ED disposition
Step 1
Intranasal
2 mcg/kg
Max 100 mcg
Intravenous
0.05 - 0.1 mg/kg
Max 4 mg if <50 kg; max 8 mg if >50 kg
Oral
10 mg/kg PO
Max 400 mg
Step 2
Ensure a true lateral XR before relying on alignment signs.


Normal alignment signs only apply when the lateral view is true.
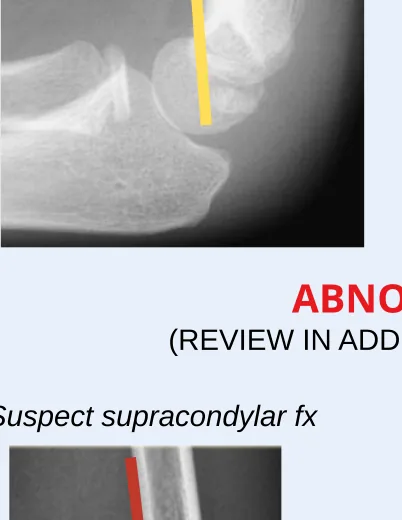
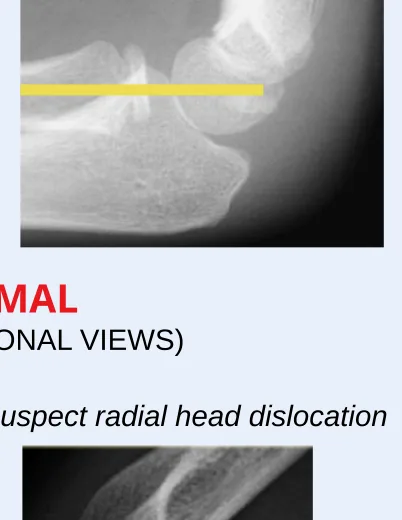

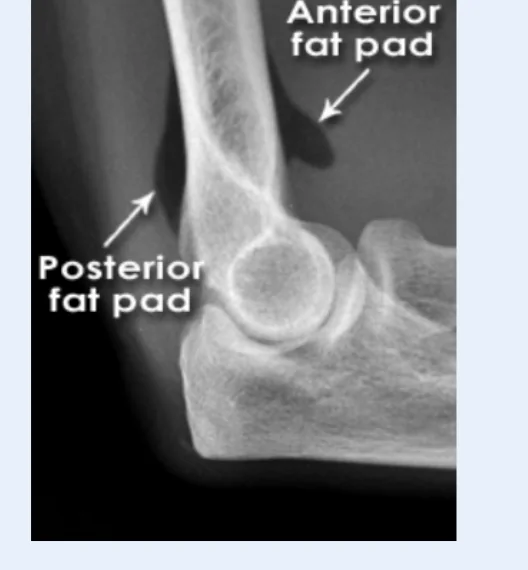
Anterior fat pad can be normal; suspect fracture with anterior sail sign or posterior fat pad.
Step 3
Type I
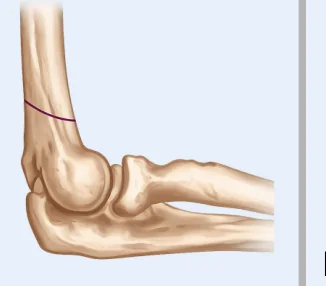
Immobilization
Disposition
Discharge for outpatient ortho
Type II
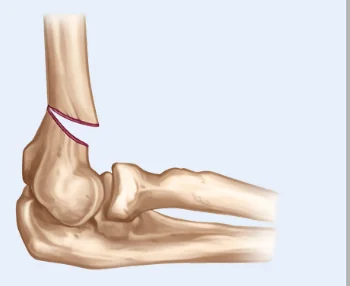
Immobilization
Disposition
Discharge with close ortho follow-up or transfer/admit for OR
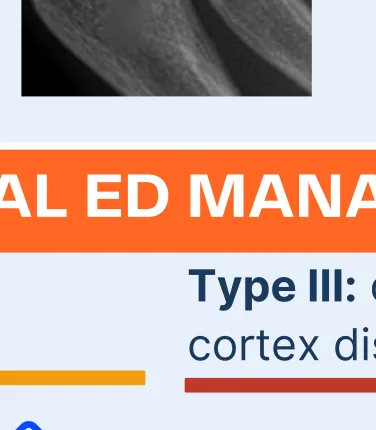
Type III
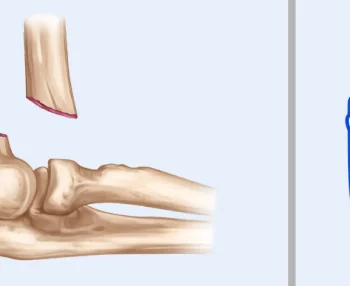
Immobilization
Disposition
Transfer/admit for OR
Step 4
Source material
Placeholder until Dana/Northwell provides the official guideline URL.